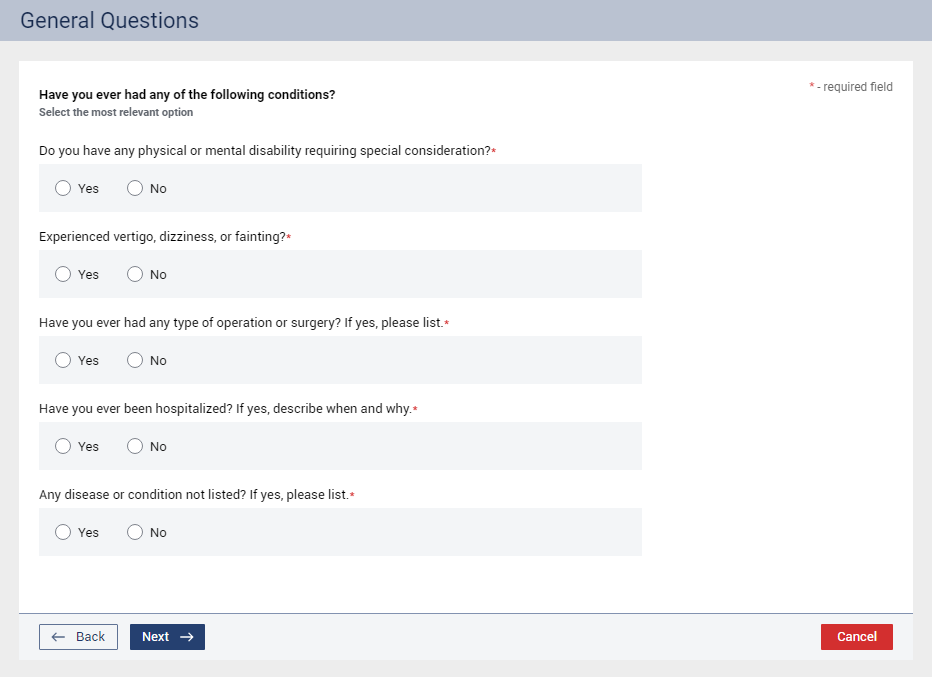
Specify if the patient has ever had any of the following conditions:
Do you have any physical or mental disability requiring special consideration? – Select Yes or No.
With Yes selected, a set of responses (Date and Description) is available.
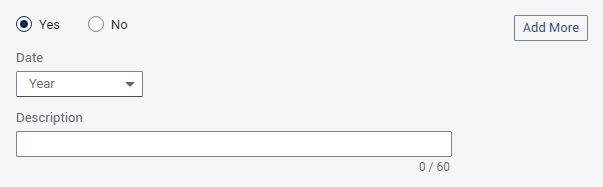
For each additional set of responses you want to add, click Add More. You can add up to four additional sets of responses.
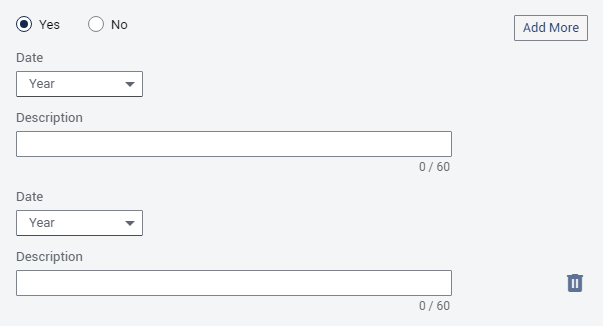
Note: To delete an additional set of responses, click the corresponding Delete button  .
.
Optionally, select a year and/or enter a description for each set of responses:
Date - Select a year or Unknown. If a year is selected, to specify that the year is approximate, select the Approximate Date checkbox.

Description - Optionally, enter up to 60 characters for the description.
Experienced vertigo, dizziness, or fainting? – Select Yes or No.
With Yes selected, a set of responses (Date and Description) is available.
For each additional set of responses you want to add, click Add More. You can add up to four additional sets of responses.
Note: To delete an additional set of responses, click the corresponding Delete button .
Optionally, select a year and/or enter a description for each set of responses:
Date - Select a year or Unknown. If a year is selected, to specify that the year is approximate, select the Approximate Date checkbox.
Description - Optionally, enter up to 60 characters for the description.
Have you ever had any type of operation or surgery? If yes, please list. – Select Yes or No.
With Yes selected, a set of responses (Date and Description) is available.
For each additional set of responses you want to add, click Add More. You can add up to four additional sets of responses.
Note: To delete an additional set of responses, click the corresponding Delete button .
Optionally, select a year and/or enter a description for each set of responses:
Date - Select a year or Unknown. If a year is selected, to specify that the year is approximate, select the Approximate Date checkbox.
Description - Optionally, enter up to 60 characters for the description.
Have you ever been hospitalized? If yes, describe when and why. – Select Yes or No.
With Yes selected, a set of responses (Date and Description) is available.
For each additional set of responses you want to add, click Add More. You can add up to four additional sets of responses.
Note: To delete an additional set of responses, click the corresponding Delete button .
Optionally, select a year and/or enter a description for each set of responses:
Date - Select a year or Unknown. If a year is selected, to specify that the year is approximate, select the Approximate Date checkbox.
Description - Optionally, enter up to 60 characters for the description.
Any disease or condition not listed? If yes, please list. – Select Yes or No.
With Yes selected, a set of responses (Date and Description) is available.
For each additional set of responses you want to add, click Add More. You can add up to four additional sets of responses.
Note: To delete an additional set of responses, click the corresponding Delete button .
Optionally, select a year and/or enter a description for each set of responses:
Date - Select a year or Unknown. If a year is selected, to specify that the year is approximate, select the Approximate Date checkbox.
Description - Optionally, enter up to 60 characters for the description.